

Enuresis
Epidemiology
- Up to 10% prevalence among 5 year olds
- Approximately 1% among individuals 15 years and older
- At age 3 to 4 years, maturation of function and control over the external urinary sphincter AND control over bladder-sphincter unit so child can voluntary initiate and inhibit micturition occurs.
- Key point 1: Provide reassurance to families and let the child know how common and normal it may be to still be wetting the bed.
- Key point 2: The longer enuresis persists, the lower probability of spontaneous resolution (i.e. older children with enuresis requires more attention and treatment)
Definitions:
- Enuresis - Intermittent incontinence while asleep in a child >= 5 years of age
- Primary enuresis - nighttime wetting in a child who has not been dry for at least 6 months
- Secondary enuresis - return of nighttime wetting after a child has been dry for at least 6 months
- Monosymptomatic enuresis - Enuresis with no other lower urinary tract symptoms (LUTS) and limited to nighttime enuresis
- Non-monosymptomatic enuresis - Enuresis with other, mainly daytime, LUTS
- Nocturia - Nighttime awakening to void
- Nocturnal enuresis - nighttime incontinence
History
- Day vs nocturnal enuresis
- # episodes bedwetting per week
- Fluid intake (especially in the evening or night)
- Juice, caffeine, or alcohol intake (especially soda, teas, and energy drinks!)
- Constipation
- Fecal incontinence - not due to insufficient wiping of the bottom
Red Flag History***
Presence of one or more suggestive for underlying bladder dysfunction (consider sending straight to Urology)
- Leakages of urine during the day
- Intermittent or continuous leakage
- Urinary frequency (>= 8x/day)
- Sudden and urgent need to urinate
- Holding maneuvers observed (e.g. Vincent's curtsey - pressing heel into perineum, leg crossing, standing on tiptoes)
- Straining to urinate
- Interrupted urinary stream or several voids, one after another
- History of recurrent urinary tract infections
- Associated neurologic symptoms
Physical Exam
Goal: 1) Confirm normal anatomy 2) look for anatomic abnormalities 3) look for neurologic abnormalities
Genital Exam
- Check underwear - signs of fecal incontinence
- Physical abnormalities (e.g. phimosis, labial adhesions)
Back Exam
- Spinal dysraphism (e.g. dimple, hemangioma, lipoma, patch of hair, sacral agenesis)
- Scoliosis (another potential sign of spinal dysraphism)
Neuro Exam
- Muscle atrophy
- Abnormal gait
- Lower extremity weakness
MSK Exam
- Foot deformities (high arch, hammer toes, clubfoot/equinovarus, limb-length discrepancies)
- Tight heel cords (can be sign of spasticity)
Labs/Tests
- Urinalysis (assess for glycosuria or signs of infection)
- +/- Urine culture
Management
If non-monosymptomatic enuresis and/or signs of LUTS, refer to Urology!
Monosymptomatic enuresis can be treated by a general practitioner using:
1) Treat any coexisting constipation FIRST
2) Restriction of fluid and diuretic intake around bedtime (no fluids after dinner or limit no more than 1 glass before bedtime)
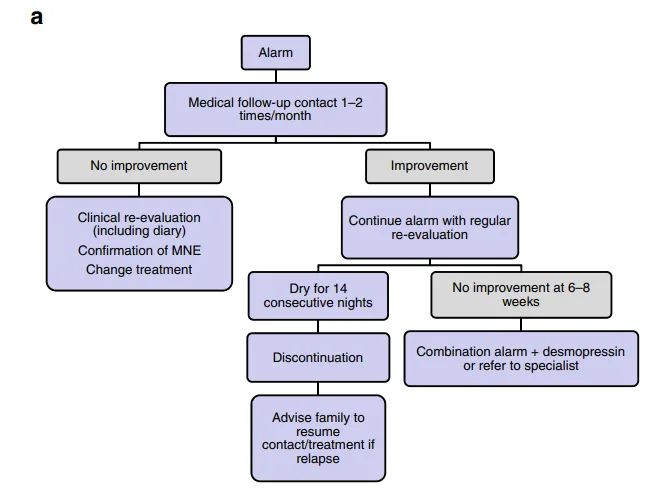
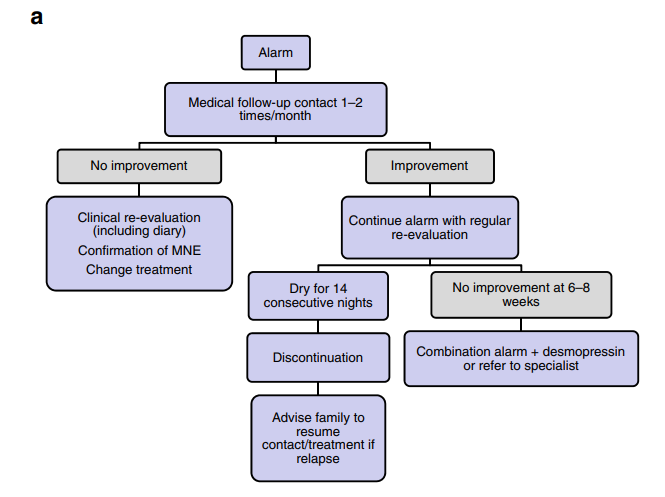
3) Bedwetting alarm
- Consistence is KEY
- Trial for 6-8 weeks DAILY
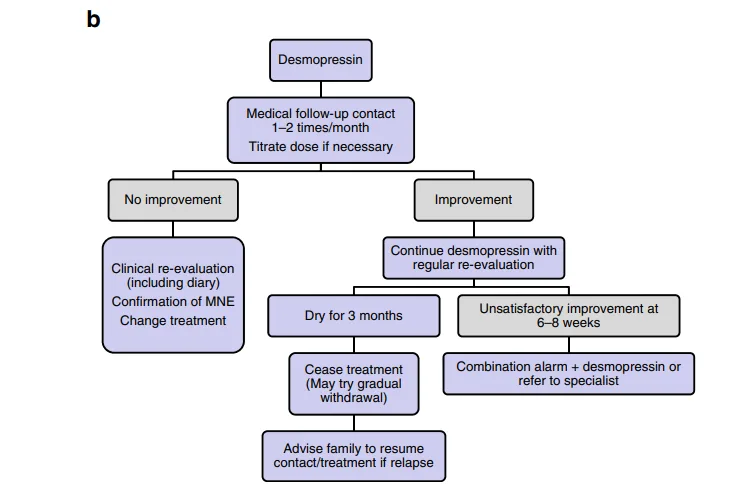
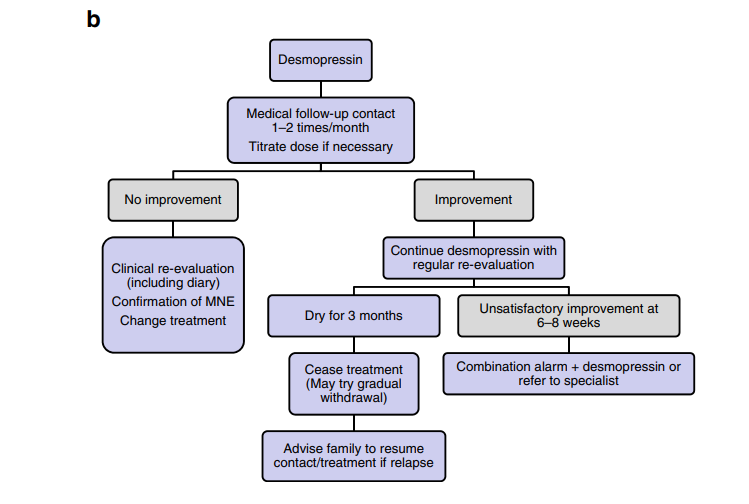
4) Desmopressin acetate
- Recommended starting dose 0.2 mg PO administered 1 hours prior to bedtime
- Titrate up to 0.4 mg-0.6 mg daily based upon clinical response (dosage is individualized for each patient)
- Limit fluid intake to a minimum from 1 hour before administration (no fluids after dinner), and until the next morning, or at least 8 hours after administration
- Precaution: Hyponatremia from antidiuretic effect of desmopressin which may lead to water intoxication and potential seizures and fatality.
- Do not administer Desmopressin for patients during acute illnesses due to risk of fluid and/or electrolyte imbalance, or under conditions that increases water intake (exercise or hot weather)
Follow-up
If there is non-response to the alarm or desmopressin therapy, the actual diagnosis may be non-monosymptomatic enuresis and non monosymptomatic enuresis. Assess upon re-evaluation. If any suspicion for non-monosymptomatic enuresis, refer to the appropriate specialist.
Constipation is a high risk factor for enuresis and treatment resistance; it should be treated prior to managing enuresis.
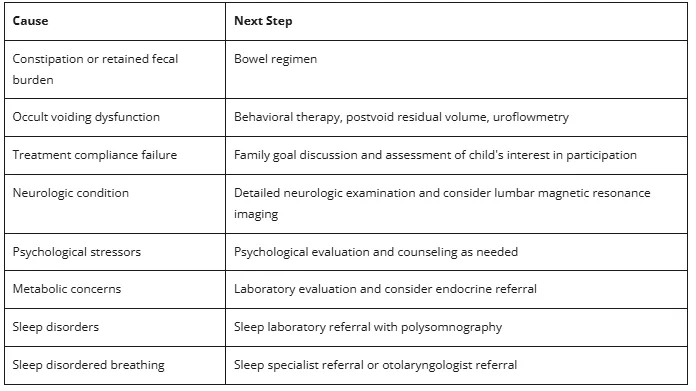
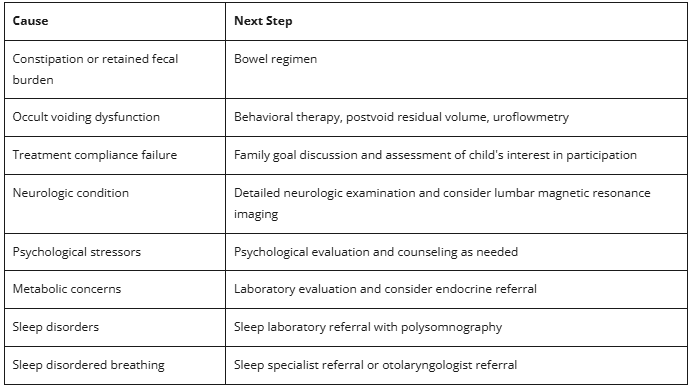
Potential Reasons for Treatment Failure
Differential Reasons for Enuresis in Children
1) Monosymptomatic enuresis
- Polyuria
- Arousal disorder (e.g. sleep disorders)
- Nocturnal detrusor overactivity (e.g. diuretics, caffeine, alcohol)
2) Non-monosymptomatic enuresis (See why you would refer to Urology?)
Functional incontinence
- Dysfunctional voiding
- Giggle incontinence
- vaginal entrapment (e.g. vaginal prolapse)
- Detrusor overactivity
Neurogenic bladder
- Spina bifida
- Tethered cord
- Sacral malformation
- Cerebral palsy
- Spinal cord tumors
- Imperforate anus
- Trauma
Anatomic abnormalities
- Exstrophy epispadias complex
- Ectopic ureter and ureterocele
- Cloacal malformations
- Urethral valve abnormalities
- Syringocele
Parental Handouts
CHOP Voiding Chart for tracking voiding
- https://www.chop.edu/sites/default/files/urology-voiding-chart-2.pdf
Information about bedwetting:
- https://www.healthychildren.org/English/health-issues/conditions/genitourinary-tract/Pages/Nocturnal-Enuresis-in-Teens.aspx?gad_source=1&gad_campaignid=69654055&gbraid=0AAAAADyMpZF-tbkbYisFeuWsGfrYiZ0wn&gclid=CjwKCAjw-J3OBhBuEiwAwqZ_h3wiBjcny9jei8xpQiThC4qnVtMkNUaHkH3-61BdEtIS7KNe3qRKDxoCCbgQAvD_BwE
Information about bedwetting alarms and how to use them:
- https://www.kidney.org/directions-your-child-when-using-bed-wetting-alarm
References
- Jonathan Apostol Guzman, Lane S. Palmer; Nocturnal Enuresis. Pediatr Rev August 2024; 45 (8): 479–481. https://doi.org/10.1542/pir.2023-006166
- https://www.ics.org/Publications/ICI_4/files-book/Comite-9.pdf
- Aaron P. Bayne, Steven J. Skoog; Nocturnal Enuresis: An Approach to Assessment and Treatment. Pediatr Rev August 2014; 35 (8): 327–335. https://doi.org/10.1542/pir.35-8-327
- https://www.accessdata.fda.gov/drugsatfda_docs/label/2019/021795s006lbl.pdf